Key Highlights
This retrospective study provides evidence that anatomical variations in upper airway fat distribution significantly influence patient comfort during transnasal office-based laryngeal surgery (OBLS). The research demonstrates that higher parapharyngeal fat volume at the palatal level correlates with lower satisfaction scores, suggesting that preoperative assessment of vocal tract anatomy may help identify patients at risk for poor procedural tolerance. These findings have important implications for patient selection and procedural planning in the growing field of awake office-based laryngeal interventions.
Background
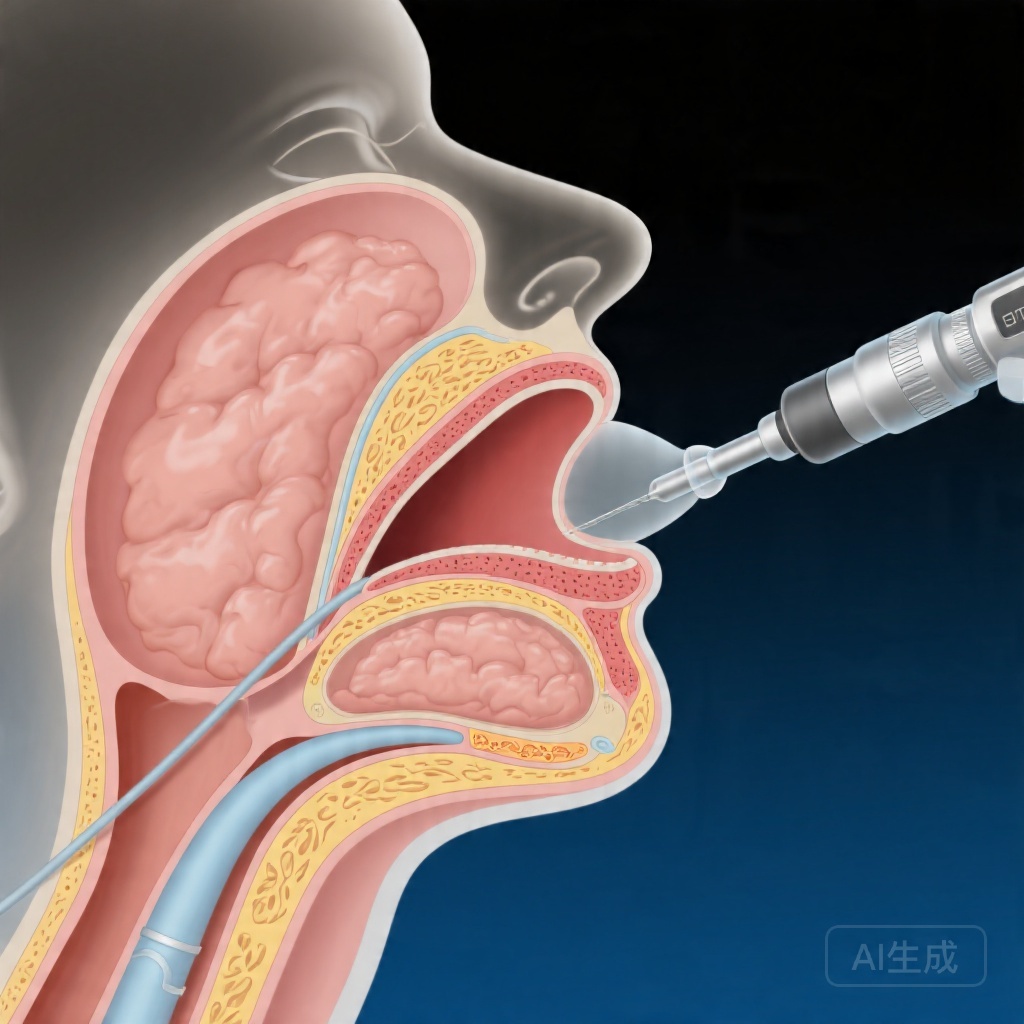
Office-based laryngeal surgery has emerged as a valuable alternative to traditional operating room procedures for selected laryngeal pathologies. Transnasal approaches offer several advantages, including reduced healthcare costs, avoidance of general anesthesia, and the ability to perform dynamic assessment of laryngeal function in an awake patient. However, the success of these procedures depends not only on technical feasibility but also on patient tolerance and comfort throughout the intervention.
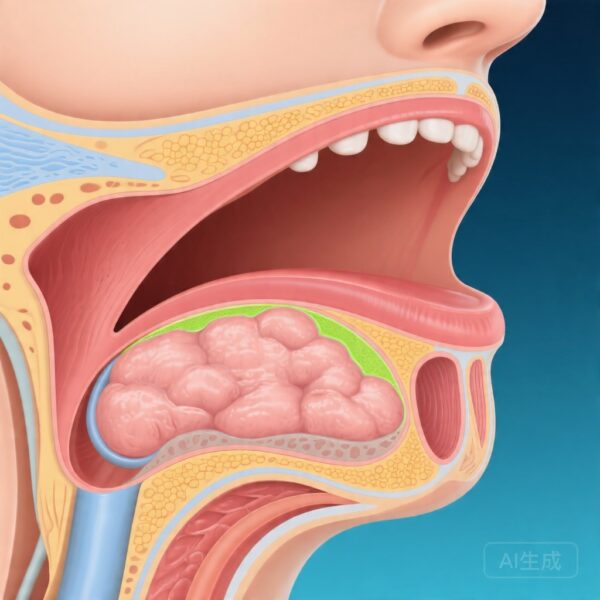
Patient comfort during transnasal OBLS is influenced by multiple factors, including nasal anatomy, gag reflex sensitivity, anxiety levels, and the experience of the operator. Recent anatomical studies have begun to explore whether structural variations in the upper airway, particularly fat distribution in the parapharyngeal space, might affect the ease of instrumentation and overall patient experience. The parapharyngeal fat pads, located lateral to the pharyngeal walls, can occupy variable volumes among individuals and may contribute to narrowing of the upper airway passage.
Understanding the relationship between vocal tract anatomy and procedural tolerance is increasingly relevant as the indications for office-based laryngeal procedures continue to expand. From vocal cord biopsies and laser procedures to injection laryngoplasty and airway dilation, the range of interventions performed in the office setting grows each year. Identifying modifiable or predictable factors that influence patient comfort could help clinicians optimize outcomes and minimize procedure abandonment or patient distress.
Study Design
This retrospective cohort study reviewed medical records and video recordings from all patients who underwent office-based laryngeal surgery via the transnasal approach between April 2024 and January 2026. The study population included 40 patients with various laryngeal pathologies requiring diagnostic or therapeutic interventions in the outpatient setting.
Three distinct fat compartments were quantified for analysis: parapharyngeal fat volume at the palatal level, parapharyngeal fat at the glossal level, and pre-epiglottic adipose tissue. These measurements were obtained from preoperative imaging or direct visualization during the procedures. Patient demographic data collected included age, gender, body mass index (BMI), smoking history, history of gastroesophageal reflux disease, and allergy history. Voice-related diagnoses and the specific type of OBLS performed were also documented.
Patient tolerance served as the primary outcome measure and was assessed using two validated instruments: the IOWA Satisfaction with Anesthesia Scale and a Visual Analog Scale (VAS) for tolerance. The IOWA scale is a multi-item questionnaire designed to assess patient satisfaction with anesthesia care during procedures, while the VAS provided a subjective 10-point rating of procedural tolerance. Statistical analysis employed linear regression modeling to examine correlations between fat compartment volumes and tolerance scores, with adjustments made for potential confounding variables including age, BMI, smoking status, and reflux history.
Key Findings
The study included 40 patients who underwent transnasal OBLS during the specified time period. The mean IOWA satisfaction score for the total cohort was 2.55 ± 0.68, while the mean VAS tolerance score was 8.70 ± 1.65. These baseline tolerance metrics indicate that, on average, patients reported reasonable satisfaction and tolerance levels, though with notable individual variation.
The primary finding of interest was a moderate, negative, statistically significant correlation between the volume of parapharyngeal fat at the palatal level and IOWA scale scores (adjusted coefficient β = -0.567, p = 0.049). This relationship persisted after controlling for potential confounders including age, BMI, smoking history, and reflux disease. The negative direction of this correlation indicates that patients with greater parapharyngeal fat volume at the palatal level tended to report lower satisfaction scores, suggesting reduced tolerance to the procedure.
When examining the relationship between palatal-level parapharyngeal fat and VAS tolerance scores, a milder negative correlation was observed (adjusted coefficient β = -0.251), though this association did not reach statistical significance (p = 0.211). The discrepancy between the IOWA and VAS findings may reflect differences in the constructs measured by these instruments, as the IOWA scale encompasses broader aspects of satisfaction with anesthesia care, while the VAS focused specifically on tolerance during the procedure.
Analysis of the other fat compartments—parapharyngeal fat at the glossal level and pre-epiglottic adipose tissue—did not reveal significant correlations with either tolerance measure in this cohort. This selective association with palatal-level fat suggests that anatomical factors at this specific location may be particularly relevant to the transnasal approach, potentially due to the narrowing effect on the nasopharyngeal passage during scope navigation.
The effect size for the primary finding, with a β coefficient of -0.567, represents a clinically meaningful association given the multifactorial nature of patient tolerance and the relatively modest sample size. The statistical significance (p = 0.049) meets conventional thresholds, though the authors appropriately acknowledge the preliminary nature of these findings pending replication in larger studies.
Expert Commentary
The study by Nasr and colleagues addresses an important yet understudied aspect of office-based laryngeal surgery—namely, how individual anatomical variations influence the patient experience. While much attention has focused on technical success rates and clinical outcomes, the subjective tolerability of these procedures deserves equal consideration, particularly as patient cooperation is essential for optimal visualization and manipulation during awake interventions.
The finding that increased parapharyngeal fat at the palatal level predicts reduced satisfaction scores has plausible mechanistic explanations. Greater fat deposition in this region may lead to relative narrowing of the nasopharyngeal corridor, requiring more manipulation to navigate the endoscope and potentially triggering greater gag reflex stimulation or mucosal contact. Additionally, patients with increased parapharyngeal fat may experience more obstruction or discomfort when the scope is advanced through this narrowed space.
The study’s retrospective design introduces inherent limitations, including potential selection bias and incomplete documentation of confounders. The sample size of 40 patients, while adequate for detecting moderate associations in this exploratory analysis, limits statistical power and precision. The authors appropriately call for larger confirmatory studies to validate these preliminary observations.
From a clinical perspective, these findings suggest that preoperative assessment of upper airway anatomy, including quantification of parapharyngeal fat, could inform patient counseling and procedural planning. Patients with substantial parapharyngeal fat deposition might benefit from additional preparation, such as topical anesthesia optimization, anxiolysis, or discussion of alternative treatment pathways if tolerance is anticipated to be poor.
The non-significant correlation with VAS scores raises questions about the sensitivity of different tolerance measurement tools and highlights the complexity of quantifying subjective patient experience. Future research should consider incorporating additional patient-reported outcomes, including pre-procedure anxiety assessments and post-procedure symptom inventories, to provide a more comprehensive picture of the patient journey.
Conclusion
This study provides initial evidence that parapharyngeal fat volume at the palatal level influences patient tolerance to transnasal office-based laryngeal surgery, with greater fat deposition associated with reduced satisfaction scores. While the findings require validation in larger cohorts, they underscore the importance of considering individual anatomical factors when selecting patients for awake office-based procedures and when counseling them about procedural expectations.
The growing demand for cost-effective, minimally invasive laryngeal interventions makes understanding the determinants of procedural success increasingly important. Future prospective studies should aim to replicate these findings, explore additional anatomical and patient-specific predictors, and develop validated algorithms for identifying patients most likely to benefit from the office-based approach versus traditional operating room procedures.
Funding and ClinicalTrials.gov
No funding source information was provided in the source material. ClinicalTrials.gov registration status was not specified.
References
1. Nasr A, Hourani R, Ghzayel L, Lababidi G, Achkar D, Sarkis V, Abou Raji Feghali P, Ghadieh J, Al Irani M, Hamdan AL. Vocal Tract Fat Distribution and Patient Tolerance to Transnasal Office-Based Laryngeal Surgery. The Laryngoscope. 2026-04-12. PMID: 41968836.