Highlights
Patients with greater parapharyngeal fat at the palatal level reported significantly lower satisfaction scores during awake laryngeal procedures.
The study identified a moderate negative correlation between palatal-level fat volume and IOWA anesthesia satisfaction scores (adjusted β = -0.567, p = 0.049).
Pre-procedure anatomical assessment may help clinicians predict patient tolerance and optimize procedural planning for transnasal office-based laryngeal surgery.
Background
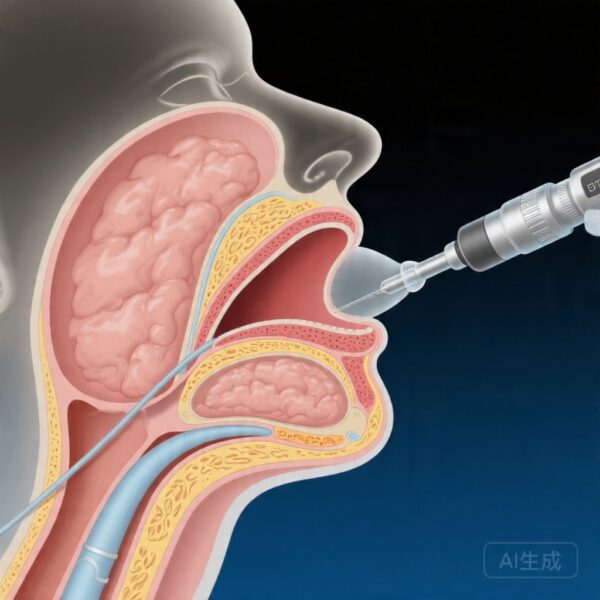
Office-based laryngeal surgery (OBLS) has emerged as a valuable alternative to operating room procedures for select diagnostic and therapeutic interventions involving the larynx and supraglottic structures. The transnasal approach offers several advantages, including avoidance of general anesthesia, reduced healthcare costs, shorter recovery times, and the ability to perform procedures in awake or minimally sedated patients. Despite these benefits, patient tolerance remains a critical determinant of procedural success, as discomfort or inadequate cooperation can compromise visualization, procedure duration, and overall outcomes.
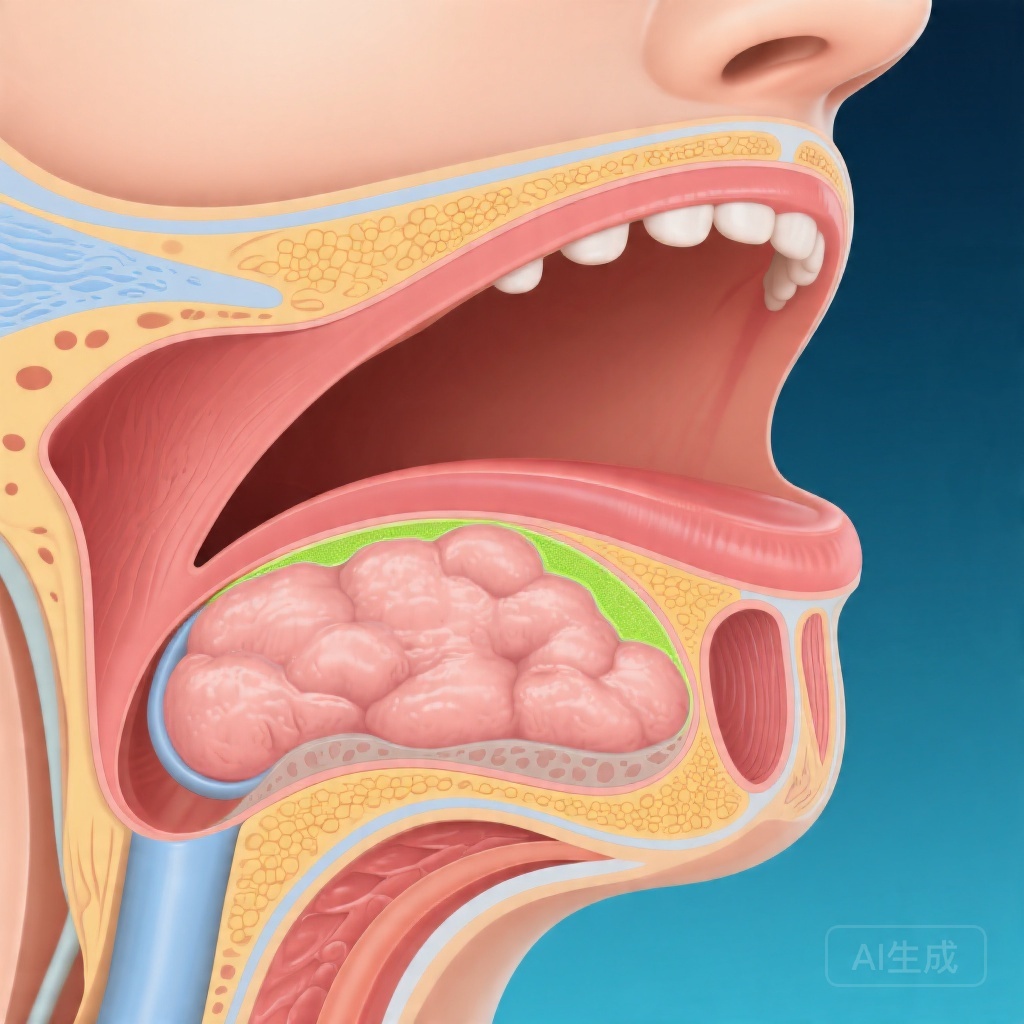
Understanding the factors that influence patient comfort during awake laryngeal surgery is therefore essential for optimizing procedural protocols and patient selection. While demographic variables such as age, body mass index, and comorbidities have been explored, the role of upper airway anatomical features—particularly fat distribution within the vocal tract—remains poorly characterized. Parapharyngeal fat pads, which occupy the spaces lateral to the pharyngeal walls, can significantly influence airway dimensions and tissue compliance. Variations in these fat compartments may affect how tissues respond to endoscopic manipulation and topical anesthesia, thereby modulating patient experience during transnasal procedures.
The present study, conducted by researchers at multiple institutions and published in The Laryngoscope, investigated whether vocal tract fat distribution correlates with patient tolerance to office-based laryngeal surgery using the transnasal approach.
Study Design
This retrospective cohort study analyzed medical records and video recordings from all patients who underwent office-based laryngeal surgery at participating institutions between April 2024 and January 2026. The study population included 40 patients who met inclusion criteria and had complete documentation for analysis.
Demographic and clinical data collected included age, gender, body mass index, smoking history, history of reflux disease, allergy status, voice diagnosis, and the specific type of OBLS performed. Three distinct fat compartments within the vocal tract were quantified using cross-sectional imaging or video endoscopy measurements: parapharyngeal fat volume at the palatal level, parapharyngeal fat at the glossal level, and pre-epiglottic adipose tissue.
Patient tolerance served as the primary outcome and was assessed using two validated instruments: the IOWA Satisfaction with Anesthesia Scale and a Visual Analog Scale (VAS). The IOWA scale provides a comprehensive evaluation of patient satisfaction across multiple domains related to anesthesia and procedural experience, while the VAS offers a simple, continuous measure of perceived tolerance. Higher IOWA scores indicate greater satisfaction, and higher VAS scores indicate better tolerance.
Statistical analysis employed linear regression modeling to evaluate correlations between fat compartment volumes and tolerance scores, with adjustments for potential confounding factors including age, BMI, smoking status, reflux history, and allergy.
Key Findings
The mean IOWA Satisfaction with Anesthesia Scale score for the total cohort was 2.55 ± 0.68, while the mean VAS tolerance score was 8.70 ± 1.65. These baseline values provide context for understanding the overall tolerability of transnasal office-based laryngeal procedures in this patient population.
The primary analysis revealed a moderate, negative, statistically significant correlation between parapharyngeal fat volume at the level of the palate and IOWA scale scores. After adjusting for confounding variables, the regression coefficient was β = -0.567 (p = 0.049), indicating that for each unit increase in palatal-level parapharyngeal fat volume, IOWA scores decreased by approximately 0.567 points. This finding suggests that greater fat accumulation in this anatomical region is associated with reduced patient satisfaction during awake laryngeal surgery.
Regarding the secondary endpoint, the analysis found only a mild, negative, non-significant correlation between palatal-level parapharyngeal fat volume and VAS tolerance scores, with an adjusted coefficient of β = -0.251 (p = 0.211). The divergence between IOWA and VAS findings may reflect differences in the constructs measured by these instruments, as the IOWA scale captures multidimensional aspects of satisfaction including psychological and physiological domains, whereas the VAS focuses primarily on procedural discomfort.
Notably, the study did not report significant correlations for the other two fat compartments analyzed—parapharyngeal fat at the glossal level and pre-epiglottic adipose tissue—suggesting that the anatomical location of fat deposition may be a critical factor in determining its impact on procedural tolerance. The palatal region, which corresponds to the level of the soft palate and nasopharynx, represents a zone where tissue bulk and compliance could particularly influence endoscope passage, topical anesthesia distribution, and patient comfort during manipulation.
Expert Commentary
The findings from this investigation contribute valuable insights into the physiological and anatomical determinants of patient experience during office-based laryngeal procedures. While the relationship between obesity and upper airway pathology is well established—particularly in obstructive sleep apnea—the current study extends this knowledge to the context of awake endoscopic surgery.
Several mechanistic explanations may account for the observed association between palatal-level parapharyngeal fat and reduced tolerance. Increased fat deposition in this region could narrow the nasal passages and nasopharynx, making transnasal endoscope insertion more difficult and potentially increasing mucosal trauma or discomfort. Additionally, adipose tissue is more compliant and less elastic than muscular or mucosal structures, which may alter the distribution of topical anesthetic agents and affect their duration of action. Fat pads may also interfere with optimal positioning of the endoscope, requiring additional manipulations that could provoke gagging, pressure sensations, or anxiety in awake patients.
The statistical significance of the correlation with IOWA scores, combined with the magnitude of the adjusted β coefficient, supports the clinical relevance of this anatomical factor. However, several limitations merit careful interpretation. The sample size of 40 patients, while adequate for detecting moderate effects, may have underpowered the analysis for secondary endpoints and subgroup comparisons. The retrospective design introduces potential selection bias and limits causal inference. Furthermore, the study did not specify which types of OBLS were performed, and procedural complexity or duration may have confounded the relationship between fat volume and tolerance.
Future research should prospectively validate these findings in larger cohorts, incorporate standardized procedural protocols, and explore whether pre-procedure imaging or endoscopic assessment of parapharyngeal fat could inform patient counseling and selection for office-based versus operating room-based interventions. Investigating whether targeted interventions—such as pre-procedure anxiolytics, alternative anesthesia techniques, or gradual desensitization—could mitigate the impact of anatomical factors on tolerance would also be of considerable clinical value.
Conclusion
This study provides evidence that increased parapharyngeal fat volume at the palatal level is associated with reduced patient satisfaction during transnasal office-based laryngeal surgery, as measured by the IOWA Satisfaction with Anesthesia Scale. The moderate negative correlation suggests that anatomical factors beyond demographic characteristics and comorbidities may significantly influence procedural tolerance.
These findings have practical implications for clinical practice. Pre-procedure assessment of vocal tract anatomy, including evaluation of parapharyngeal fat distribution, could help otolaryngologists anticipate which patients may experience greater discomfort during awake laryngeal procedures. Such information could guide shared decision-making, procedural planning, and the selection of appropriate anesthesia or sedation strategies.
Larger prospective studies are needed to confirm these preliminary observations, explore mechanisms, and determine whether anatomical screening could improve patient selection and outcomes for office-based laryngeal interventions. Until then, clinicians should remain attentive to individual patient factors and be prepared to modify their approach based on real-time assessment of patient comfort.
References
1. Nasr A, Hourani R, Ghzayel L, Lababidi G, Achkar D, Sarkis V, Abou Raji Feghali P, Ghadieh J, Al Irani M, Hamdan AL. Vocal Tract Fat Distribution and Patient Tolerance to Transnasal Office-Based Laryngeal Surgery. The Laryngoscope. 2026-04-12. PMID: 41968836.