
Highlight
- Majority (84%) of children clinically diagnosed with NAFLD meet criteria for metabolic dysfunction-associated steatotic liver disease (MASLD).
- Approximately 16% of pediatric patients are reclassified due to alcohol use below adult thresholds (Met-ALD) or drug-induced liver injury.
- Adolescents have a higher prevalence (5.4%) of Met-ALD, underscoring the importance of detailed alcohol consumption assessment in this group.
- A systematic diagnostic approach incorporating metabolic risk factors, alcohol exposure, and medication history is critical for accurate diagnosis and management of pediatric steatotic liver diseases.
Study Background
Nonalcoholic fatty liver disease (NAFLD) represents the most common chronic liver disorder in children, closely linked to the rising prevalence of pediatric obesity and metabolic syndrome. Historically, diagnostic nomenclature and criteria centered around exclusion of significant alcohol intake, which is less common in children, but adult studies have noted overlapping metabolic and environmental contributors to steatotic liver disease. Recognizing limitations of the NAFLD definition, recent adult-centric consensus introduced the term steatotic liver disease (SLD), stratifying etiologies to better capture metabolic dysfunction and other contributing factors. The metabolic dysfunction-associated steatotic liver disease (MASLD) category includes patients with hepatic steatosis plus at least one cardiometabolic risk factor. Additionally, the Met-ALD category acknowledges coexistence of metabolic dysfunction and lower-level alcohol consumption that does not meet classical ALD thresholds. While these frameworks have shown strong concordance with prior NAFLD diagnoses in adults, their applicability and validity in pediatric populations remain uncertain, particularly given distinct patterns of alcohol exposure and medication use in children. This study aimed to clarify the reclassification of pediatric NAFLD cases using the SLD framework to guide diagnosis and optimize management strategies.
Study Design
This retrospective analysis utilized data from the NASH Clinical Research Network (NASH CRN), encompassing multiple U.S. centers specializing in pediatric liver disease. The cohort included 1,019 children diagnosed clinically with NAFLD who had undergone liver biopsy, with central histological review to confirm steatosis and exclude other etiologies. Detailed clinical and demographic data were collected, comprising Body Mass Index (BMI), alcohol consumption (noting quantity against defined adult thresholds), and exposure to hepatotoxic medications. Patients were reclassified into steatotic liver disease subtypes based on the presence of cardiometabolic risk factors, minimal alcohol exposure, or medication-related liver injury, following the new MASLD and Met-ALD criteria. The primary endpoint was the proportion of children fitting MASLD criteria versus other subgroups. Secondary analyses considered risk factor distributions and age-related patterns.
Key Findings
Among the 1,019 pediatric patients initially diagnosed with NAFLD, 858 (84%) met MASLD criteria, confirming metabolic dysfunction as the dominant driver of steatotic liver disease in children. On average, participants had 2.7 (±1.1) cardiometabolic risk factors, highlighting the multifactorial nature of their liver disease; 41 children (4.7%) met all five assessed cardiometabolic risk factors, underscoring severe metabolic involvement in subsets.
TABLE 1.
Characteristics of study participants
| Participant characteristic | Total, N=1019 | MASLD, N=858 | NAFLD not MASLD, N=161 | p |
|---|---|---|---|---|
| Age, y, mean (SD) | 13.0 (2.8) | 12.8 (2.8) | 14.3 (2.6) | <0.001 |
| Sex, N (%) | 0.88 | |||
| Male | 723 (71) | 608 (71) | 115 (71) | |
| Female | 296 (29) | 250 (29) | 46 (29) | |
| Ethnicity, N (%) | <0.001 | |||
| Hispanic | 735 (72) | 654 (76) | 85 (53%) | |
| Anthropometrics | ||||
| Weight, kg, mean (SD) | 83.1 (25.9) | 81.5 (25.1) | 91.2 (28.4) | <0.001 |
| Height, cm, mean (SD) | 1.59 (0.14) | 1.58 (0.14) | 1.64 (0.14) | <0.001 |
| BMI, mean (SD) | 32.2 (6.4) | 32.0 (6.2) | 33.3 (7.2) | 0.02 |
| BMI z-score, mean (SD) | 2.9 (1.4) | 3.0 (1.3) | 2.9 (1.6) | 0.68 |
| Systolic blood pressure, mm Hg, mean (SD) | 120 (13) | 120 (13) | 121 (12) | 0.66 |
| Diastolic blood pressure, mm Hg, mean (SD) | 68 (9) | 68 (9) | 68 (10) | 0.83 |
| Laboratory values | ||||
| AST, U/L, mean (SD) | 64 (54) | 65 (55) | 60 (48) | 0.35 |
| ALT, U/L, mean (SD) | 111 (103) | 113 (104) | 102 (96) | 0.43 |
| ALP, U/L, mean (SD) | 224 (105) | 230 (103) | 188 (109.7) | <0.001 |
| GGT, U/L, mean (SD) | 46 (41) | 45 (37) | 52 (59) | 0.07 |
| Total bilirubin, mg/dL, mean (SD) | 0.51 (0.29) | 0.50 (0.28) | 0.55 (0.33) | 0.06 |
| Platelet count, 103 cells/mcl, mean (SD) | 293 (70) | 296 (70) | 276 (68) | 0.001 |
| Triglycerides, mg/dL, mean (SD) | 148 (80) | 147 (76) | 155 (97) | 0.21 |
| Total cholesterol, mg/dL, mean (SD) | 164 (36) | 164 (36) | 165 (37) | 0.77 |
| HDL, mg/dL, mean (SD) | 39 (9) | 39 (9) | 40 (11) | 0.71 |
| LDL, mg/dL, mean (SD) | 96 (30) | 97 (30) | 96 (31) | 0.72 |
| Glucose, mg/dL, mean (SD) | 91 (22) | 92 (22) | 89 (24) | 0.28 |
| HbA1c, %, mean (SD) | 5.5 (0.8) | 5.5 (0.8) | 5.5 (0.9) | 0.98 |
| PNPLA3 genotype, N (%) | <0.001 | |||
| CC | 107 (15) | 79 (13) | 28 (23) | |
| CG | 252 (34) | 192 (31) | 60 (49) | |
| GG | 377 (51) | 343 (56) | 34 (28) | |
| Histology | ||||
| Definite steatohepatitis, N (%) | 190 (19) | 162 (19) | 28 (24) | 0.20 |
| Fibrosis stages 2–4, N (%) | 268 (26) | 233 (27) | 35 (22) | 0.15 |
| Ballooning, grade 2, N (%) | 86 (8) | 70 (8) | 16 (10) | 0.46 |
Importantly, 33 children (3.2%) qualified for the Met-ALD category due to both steatosis with metabolic dysfunction and alcohol intake below adult ALD thresholds. Notably, this prevalence increased to 5.4% in adolescents, reflecting an age-dependent pattern of alcohol exposure even within pediatric populations. This finding emphasizes the need to incorporate detailed lifestyle and alcohol-use assessments during pediatric liver disease evaluation.
FIGURE 2.

Reclassification of children with NAFLD using the SLD framework. This pie chart illustrates the distribution of diagnostic categories among children initially diagnosed with NAFLD following reclassification under the updated steatotic liver disease (SLD) framework. The majority met criteria for metabolic dysfunction–associated steatotic liver disease (MASLD), while others were reclassified based on alcohol use (Met-ALD, ALD), exposure to hepatotoxic medications (DISLD), or absence of metabolic risk factors (cryptogenic SLD). A subset was excluded from SLD classification due to insufficient hepatic steatosis or alternative etiologies, including microvesicular steatosis (n=9) and viral hepatitis (n = 1). Percentages represent the proportion of the total cohort assigned to each diagnostic category. Abbreviations: ALD, alcohol-associated liver disease; DISLD, drug-induced steatotic liver disease; MASLD, metabolic dysfunction–associated steatotic liver disease; Met-ALD, Metabolic dysfunction and alcohol-associated steatotic liver disease; SLD, steatotic liver disease.
FIGURE 3.
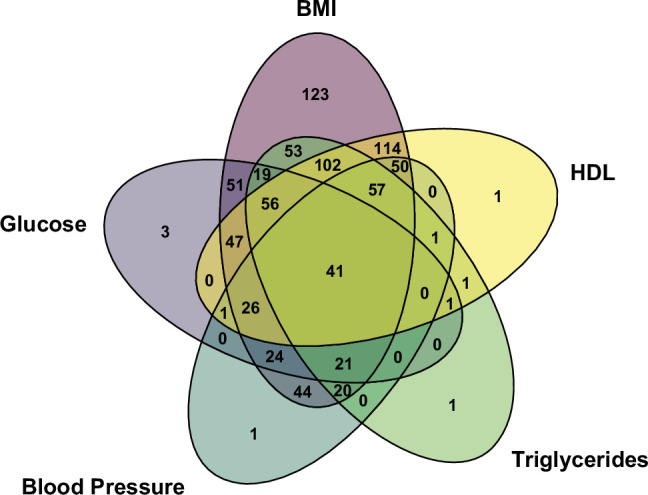
Distribution of cardiometabolic risk factors among children with MASLD. This Venn diagram illustrates the overlap and distribution of five cardiometabolic risk factors among children diagnosed with MASLD.
Additionally, 66 children (6.5%) were reclassified as having drug-induced steatotic liver disease due to exposure to known hepatotoxic medications, highlighting a clinically relevant subgroup often overlooked under traditional NAFLD definitions.
Thus, nearly one in six children initially diagnosed with NAFLD were reclassified under the updated steatotic liver disease framework based on these additional etiological considerations.
Expert Commentary
This multicenter study provides pivotal insights into the evolving landscape of pediatric steatotic liver disease classification. By applying the adult-informed SLD nomenclature to a large biopsy-confirmed pediatric cohort, the study demonstrates that while metabolic dysfunction remains the principal factor, alcohol and medication-induced injury are important contributors warranting dedicated diagnostic consideration. These findings align with growing recognition that pediatric liver disease is heterogeneous and that simplistic exclusion-based definitions may overlook critical determinants.
Importantly, the identification of Met-ALD in adolescents challenges assumptions that alcohol is negligible in pediatric liver disease etiology, underscoring the need for systematic, validated screening tools for alcohol use in this age group. Furthermore, the prevalence of drug-induced steatotic liver injury highlights the importance of thorough medication histories and awareness of emerging hepatotoxic agents in pediatrics.
Limitations include retrospective design and reliance on adult-derived alcohol thresholds that may not perfectly map to pediatric physiology or behavioral patterns. Additionally, the NASH CRN recruitment may lead to selection bias towards more severe disease phenotypes. Despite these, the study’s multicenter nature and centralized histological assessment strengthen its generalizability.
Future work should prospectively validate pediatric-specific steatotic liver disease definitions, explore the mechanistic underpinnings of Met-ALD and drug-induced SLD in children, and integrate these insights into clinical guidelines to optimize individualized care.
Conclusion
The transition from the NAFLD diagnostic framework to the steatotic liver disease paradigm in pediatrics reveals that most children still fit the MASLD profile with metabolic dysfunction driving pathology. However, a substantial minority’s disease etiology includes modest alcohol exposure (Met-ALD) or drug-induced injury, warranting more nuanced diagnostic strategies. This reclassification has significant implications for clinical assessment, management, and counseling in pediatric steatotic liver disease, emphasizing the necessity of comprehensive evaluation encompassing metabolic risk assessment, alcohol use inquiry, and medication history. Integrating the steatotic liver disease framework may enhance precision in diagnosis and therapeutic targeting, ultimately improving outcomes for affected children.
Funding and ClinicalTrials.gov
The study was supported by the NASH Clinical Research Network under grants from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Specific funding details and conflicts of interest were outlined in the original publication. There was no prospective clinical trial registration required for this retrospective analysis.
References
1. Lam TBN, Yates KP, Noon SL, Newton KP, Fishbein MH, Molleston JP, Xanthakos SA, Jain AK, Vos MB, Blondet NM, Mysore KR, Behling CA, Wilson LA, Schwimmer JB; and the NASH CRN. Reclassifying pediatric NAFLD using the steatotic liver disease framework: A multicenter retrospective study from the NASH CRN. Hepatology. 2026 Jul 1;84(1):129-142. doi: 10.1097/HEP.0000000000001577. Epub 2025 Oct 17. PMID: 41104541; PMCID: PMC13070534.
2. Eslam M, Sanyal AJ, George J. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999-2014.e1.
3. Vos MB, Abrams SH, Barlow SE, et al. NASPGHAN Clinical Practice Guideline for the diagnosis and treatment of nonalcoholic fatty liver disease in children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J Pediatr Gastroenterol Nutr. 2017;64(2):319-334.
4. Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73-84.
5. Schwimmer JB, Celedon MA, Lavine JE, et al. Incomplete alcohol abstinence in adolescent alcohol-related liver disease and implications for extended classification. J Pediatr Gastroenterol Nutr. 2024;78(3):442-449.

