Introduction
Patients with type 2 diabetes (T2D) face numerous health challenges, especially when developing infections such as urinary tract infections (UTIs). Recent studies suggest that the initiation of SGLT2 inhibitors soon after a UTI diagnosis can significantly affect long-term health outcomes. This article explores the association between SGLT2 inhibitors and improved survival rates in T2D patients following a UTI diagnosis.
Methodology
UTIs, along with conditions like acute pyelonephritis, are not only common but also serious complications for individuals suffering from T2D. Following these infections, patients are often at an elevated risk for systemic complications, decreased kidney function, and cardiovascular issues.
To investigate the potential benefits of SGLT2 inhibitors, researchers conducted a retrospective cohort study utilizing global health network data spanning from 2016 to 2023. The primary aim was to determine whether starting SGLT2 inhibitors within three months of a UTI diagnosis leads to better long-term health outcomes when compared to starting DPP-4 inhibitors.
The study included a total of 4,258 adults with T2D who were matched based on propensity scores. In this cohort, 2,129 individuals initiated SGLT2 inhibitors, while another 2,129 began treatment with DPP-4 inhibitors. The mean age of participants was approximately 61 years, with a gender distribution of around 28%-29% male.
The primary outcome of interest was mortality, while secondary outcomes included the incidence of major adverse kidney events and major adverse cardiovascular events over a four-year follow-up period.
Findings
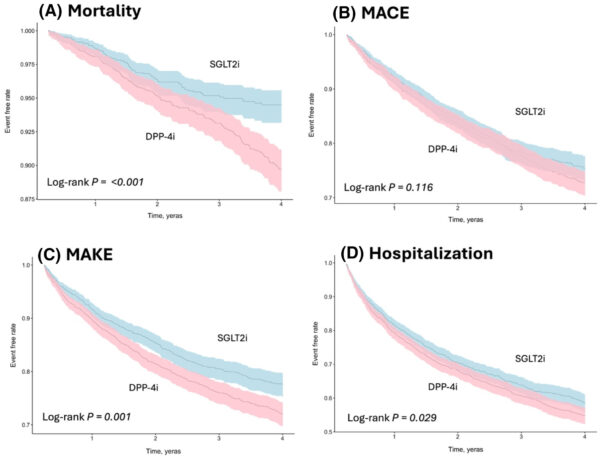
The results revealed that the use of SGLT2 inhibitors was linked to a 41% reduction in the risk of mortality compared to those taking DPP-4 inhibitors (hazard ratio [HR], 0.59; 95% confidence interval [CI], 0.45-0.77). This effect was notably stronger among certain patient demographics—women, younger patients under 65 years, those with an A1c level of 7% or higher, and individuals without existing cardiovascular or ischemic heart diseases.
Moreover, the beneficial effects of SGLT2 inhibitors on mortality outcomes began to manifest as early as six months following the UTI diagnosis. Alongside improved mortality rates, there was also a notable decrease in the risk of major adverse kidney events (HR, 0.784; 95% CI, 0.682-0.900) linked to SGLT2 inhibitors. However, no significant differences were observed regarding major adverse cardiovascular events.
Interestingly, the recurrence of UTIs was found to be slightly lower in patients using SGLT2 inhibitors compared to those on DPP-4 inhibitors. Additionally, SGLT2 inhibitors were associated with lower risks for hospital admissions, dependency on dialysis, sepsis, and emergency department visits.
Conclusion and Practice Implications
These findings underscore the importance of considering SGLT2 inhibitors as a frontline therapeutic option within the first few months post-UTI diagnosis in T2D patients. The authors encourage clinicians to prioritize early initiation of SGLT2 inhibitors, given their safety and effectiveness in improving patient outcomes.
As such, for healthcare providers treating patients with T2D, these insights emphasize the need for greater awareness of the benefits associated with SGLT2 inhibitors in the context of post-infection management.
Reference
Wang HW, Tsai MH, Fang YW, Lu KC, Wang J, Lu CL. Association between sodium-glucose cotransporter 2 inhibitor use and clinical outcomes in patients with type 2 diabetes after urinary tract infection. Diabetes Obes Metab. 2025 Aug 4. doi: 10.1111/dom.70003 IF: 5.7 Q1 . Epub ahead of print. PMID: 40757430 IF: 5.7 Q1 .

