– A randomized, single‑blinded, parallel‑group trial (RICBP‑EH, NCT05910242) enrolled 102 patients with essential hypertension (SBP ≥140 mm Hg) and compared 7 days of remote ischemic conditioning (RIC) versus sham RIC.
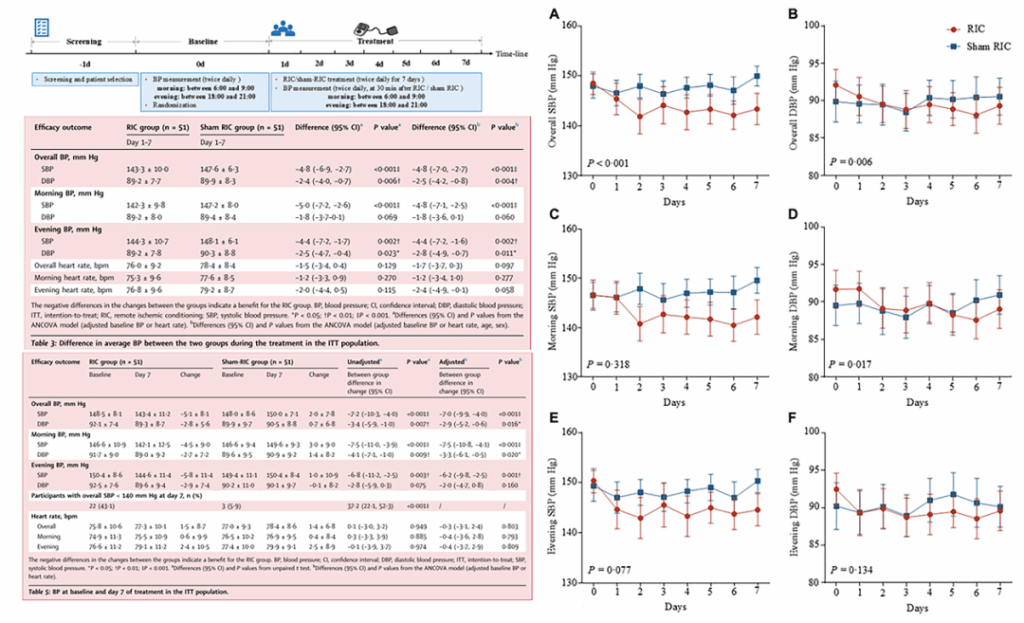
– The RIC group achieved a lower average systolic blood pressure (SBP) during treatment: 143.3 ± 10.0 vs 147.6 ± 6.3 mm Hg (baseline‑adjusted difference −4.8 mm Hg; 95% CI −6.9 to −2.7; P < 0.001).
– By day 7 the between‑group reduction in overall SBP favored RIC (between‑group difference −7.2 mm Hg; 95% CI −10.3 to −4.0; P < 0.001). Treatment was well tolerated with no major adverse events.
Background and clinical importance
Uncontrolled arterial hypertension remains one of the leading modifiable cardiovascular risk factors worldwide. A substantial proportion of patients with essential hypertension have insufficient BP control despite available pharmacotherapies, lifestyle measures, or limited adherence. Non‑pharmacologic adjuncts that are safe, low‑cost, and easy to deliver could help improve blood pressure control at the population level.
Remote ischemic conditioning (RIC) is a procedure in which brief, reversible episodes of ischemia are applied to a limb (typically by inflation of a blood‑pressure cuff) to trigger systemic protective responses. RIC has been investigated primarily for myocardial and cerebral ischemia protection; smaller translational and clinical studies have also reported effects on endothelial function, autonomic tone, and inflammation — pathways potentially relevant to BP regulation.
Study design
RICBP‑EH was a randomized, single‑blinded, parallel‑group trial conducted at a single centre in Changchun, China (ClinicalTrials.gov NCT05910242). Key elements:
Population: adult patients with clinically diagnosed essential hypertension and sitting systolic BP ≥140 mm Hg. This included people with SBP ≥140 mm Hg despite antihypertensive therapy as well as untreated individuals with SBP ≥140 mm Hg.
Intervention: remote ischemic conditioning (RIC) applied for 7 consecutive days.
Comparator: sham RIC applied for the same schedule for blinding.
BP measurement: sitting blood pressure measured twice daily (morning 06:00–09:00 and evening 18:00–21:00) from the day before treatment to the final day (8 days total; 16 readings per participant). The primary endpoint was the difference in average SBP during the treatment period (7 days, 14 measurements).
Analysis: intention‑to‑treat analysis included all randomly assigned participants; adverse events were recorded.
Key findings
Between June 20, 2023, and March 6, 2024, 102 patients completed the study (n = 51 per arm). Principal results are summarized below.
Primary outcome
The average SBP during the 7‑day treatment period was significantly lower in the RIC group than the sham group (143.3 ± 10.0 vs 147.6 ± 6.3 mm Hg). After adjustment for baseline SBP, the between‑group difference was −4.8 mm Hg (95% CI −6.9 to −2.7 mm Hg; P < 0.001) in the intention‑to‑treat analysis.
Temporal pattern and day‑7 change
The trend of overall SBP (daily average of morning and evening SBP) over time showed a statistically significant group‑by‑time interaction (F = 4.316, P < 0.001), indicating divergent trajectories between groups. The reduction from baseline to day 7 in overall SBP was larger in the RIC group than in the sham group (−5.1 ± 8.1 vs +2.0 ± 7.8 mm Hg), yielding a between‑group difference of −7.2 mm Hg (95% CI −10.3 to −4.0 mm Hg; P < 0.001).
Safety and tolerability
No major adverse events were reported. The number of adverse events did not differ significantly between groups. The short daily RIC protocol was generally well tolerated across the study population.
Clinical interpretation and magnitude of effect
A randomized reduction in average SBP of approximately 4.8 mm Hg during the treatment week, and a day‑7 between‑group difference of about 7.2 mm Hg, is clinically notable. Even modest SBP reductions can translate into meaningful reductions in cardiovascular risk over time. From a practical standpoint, RIC represents a non‑pharmacologic, device‑based adjunct that could be applied at home or in outpatient settings if longer‑term efficacy and durability are shown.
It is important to emphasize that this study measured short‑term BP responses (7 days). Whether the observed BP lowering persists with continued RIC, and whether it confers reductions in hard cardiovascular outcomes, remains unknown.
Strengths of the trial
Randomized, controlled design with intention‑to‑treat analysis.
Frequent standardized BP measurements (twice daily) allowing a robust estimate of short‑term BP effects and within‑subject variability assessment.
Use of a sham RIC arm improves internal validity by controlling for nonspecific effects and expectation.
Careful reporting of adverse events suggests acceptable short‑term safety.
Limitations and considerations
Short duration: the intervention lasted 7 days. Hypertension management is chronic; durability of BP lowering with sustained RIC or optimal dosing regimens remains unknown.
Single‑centre and ethnically homogeneous population (China): generalizability to other healthcare settings and ethnic groups requires validation in multicentre, multiethnic cohorts.
Single‑blinded design: the trial was single‑blinded (participants or investigators not both); residual bias in measurements or behavior cannot be fully excluded.
Mechanistic data were not reported: the biological pathways mediating BP reduction (autonomic modulation, endothelial function, inflammatory mediators, neurohormonal changes) were not delineated and warrant mechanistic studies.
Comparator details: while a sham arm was used, the report does not give exhaustive detail on blinding fidelity (e.g., success of participant masking), which is relevant for device and procedural trials.
Biological plausibility and potential mechanisms
Several mechanisms may explain how limb RIC could lower BP. Experimental and early clinical data suggest RIC can improve endothelial function, increase nitric oxide bioavailability, modulate autonomic balance with relative enhancement of parasympathetic activity, and attenuate systemic inflammation — each of which could lower peripheral vascular resistance or reduce central sympathetic drive. RIC might also influence vascular stiffness, which is particularly relevant in older patients with systolic hypertension. These mechanisms remain speculative in the context of BP control and require targeted mechanistic studies using vascular function testing, autonomic profiling, and biomarker analysis.
Implications for practice and research
At present, RIC should be considered an experimental adjunct for BP lowering rather than an established therapy. The RICBP‑EH trial provides important proof‑of‑concept evidence that short‑term RIC reduces SBP in patients with uncontrolled essential hypertension and is well tolerated. Steps needed before clinical implementation include:
Replication in larger, multicentre trials with more diverse populations.
Longer‑term studies to determine durability of effect, optimal dosing frequency/duration, and adherence in outpatient settings.
Mechanistic substudies to identify responders, refine patient selection, and understand pathways to guide combination with pharmacologic therapies.
Cost‑effectiveness analyses and pragmatic implementation studies to assess feasibility of home‑based RIC programs.
Conclusion
RICBP‑EH is the first randomized controlled study to demonstrate that short‑term remote ischemic conditioning lowers systolic blood pressure in patients with essential hypertension and SBP ≥140 mm Hg, with an adjusted treatment effect of approximately −4.8 mm Hg during the 7‑day intervention and no major safety signals. The findings are promising and support further investigation of RIC as a potential low‑risk adjunctive therapy for patients with suboptimally controlled blood pressure, but larger and longer trials with mechanistic endpoints are required before RIC can be recommended in routine practice.
Funding and trial registration
Funding: National Natural Science Foundation of China; Science and Technology Department of Jilin Province; Jilin Provincial Key Laboratory; Norman Bethune Health Science Center of Jilin University; Talent Reserve Program of the First Hospital of Jilin University; Science and Technology Research Program of the Education Department of Jilin Province.
ClinicalTrials.gov registration: NCT05910242.
Selected references
1. Yin WJ, Wang SJ, Qu Y, Ren JX, Zhang P, Abuduxukuer R, Yang Y, Guo ZN. Efficacy of remote ischemic conditioning on blood pressure in essential hypertension in China (RICBP‑EH): a randomised, controlled, parallel‑group trial. EClinicalMedicine. 2025 Oct 16;89:103562. doi: 10.1016/j.eclinm.2025.103562 . PMID: 41146928 ; PMCID: PMC12554178 .
2. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J Am Coll Cardiol. 2018;71:e127–e248.
3. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104.
Author note
This article summarizes and interprets the RICBP‑EH randomized trial for clinicians and researchers. It does not replace detailed reading of the original trial report for methodological specifics and is intended to stimulate further clinical and mechanistic research on RIC for blood pressure control.