Acute ischemic stroke due to large vessel occlusion represents a critical neurological emergency, where successful recanalization through endovascular thrombectomy (EVT) markedly improves outcomes. Despite advances leading to near 90% reperfusion success rates, the optimal management of post-EVT blood pressure (BP) remains uncertain. Elevated BP after EVT is common and may influence reperfusion injury and hemorrhagic transformation. Intravenous antihypertensives are frequently employed to control BP in this setting; however, their independent impact on functional recovery after EVT is inadequately defined. This secondary analysis of the OPTIMAL-BP trial investigates the association between intravenous antihypertensive administration and functional outcomes following successful EVT in acute ischemic stroke patients.
Study Design
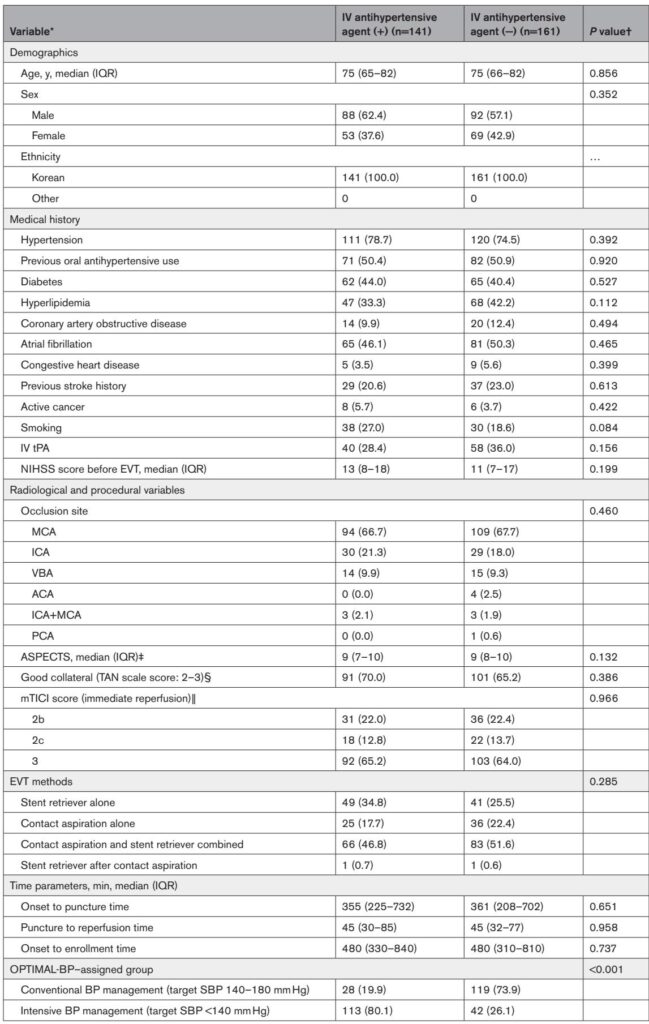
The OPTIMAL-BP trial was a multicenter, randomized, open-label trial with blinded endpoint assessment, enrolling 302 acute ischemic stroke patients with large vessel occlusion treated with EVT across 19 South Korean centers from June 2020 to November 2022. Eligible patients had successful reperfusion and elevated systolic blood pressure (SBP ≥ 140 mm Hg) within 2 hours post-EVT. They were randomized to intensive BP control (target SBP <140 mm Hg) or conventional control (target SBP 140–180 mm Hg). Intravenous antihypertensive administration, predominantly nicardipine, was initiated to achieve target BP levels. Patients were classified according to intravenous antihypertensive use within 24 hours post-enrollment, irrespective of dosage or duration. The primary efficacy outcome was functional independence at 3 months (modified Rankin Scale [mRS] score 0–2), with safety outcomes including symptomatic intracerebral hemorrhage (ICH) and stroke-related mortality.
Key Findings
Among 302 patients (median age, 75 years; 59.6% male), 141 (46.7%) received intravenous antihypertensives within 24 hours after EVT. Nicardipine was utilized in 94.3% of treated patients. Notably, patients receiving intravenous antihypertensives were predominantly assigned to the intensive BP management group (80.1%).
Despite achieving similar mean SBP over 24 hours, those treated with intravenous antihypertensives exhibited significantly lower rates of functional independence at 3 months (39.0% vs 53.4%; adjusted odds ratio [AOR] 0.51; 95% CI, 0.27–0.95; P=0.035) and higher stroke-related mortality (9.9% vs 3.7%; AOR, 4.21; 95% CI, 1.24–16.4; P=0.027). Symptomatic ICH incidence did not differ significantly between groups (10.6% vs 6.8%; P=0.267).
Secondary analyses revealed worse mRS score distribution and lower rates of excellent neurological recovery at 24 hours (AOR 0.46; 95% CI, 0.22–0.94; P=0.036) in the intravenous antihypertensive group. There was no difference in reperfusion success, infarct volume, or quality of life metrics. Dose-response analysis suggested a linear trend associating higher total dose and longer duration of intravenous antihypertensive use with reduced functional independence.
Subgroup analyses showed a consistent unfavorable association across predefined strata, and sensitivity models confirmed robustness of results. Timing of antihypertensive initiation (within 60, 90, or 120 minutes after reperfusion) did not significantly affect outcomes.
An exploratory analysis restricted to patients maintaining SBP between 140 and 180 mm Hg affirmed that intravenous antihypertensive use correlated with poorer functional independence (42.5% vs 58.9%; AOR 0.47; 95% CI, 0.23–0.96; P=0.040) and increased mortality (8.0% vs 2.8%; AOR 12.3; 95% CI, 1.71–162; P=0.027), with trends toward worse neurological outcomes and increased malignant cerebral edema.
Expert Commentary
This analysis uniquely elucidates the independent association of intravenous antihypertensives with adverse functional outcomes after EVT, suggesting potential harm beyond targeted BP levels. Intravenous agents, often rapid-acting like nicardipine, may induce abrupt BP drops that compromise cerebral perfusion in the vulnerable penumbra during impaired autoregulation post-recanalization. Prior randomized controlled trials focusing on BP targets have similarly observed that intensive BP lowering does not reduce symptomatic ICH but may worsen outcomes.
Persistence of no-reflow phenomena despite successful macrovascular recanalization may render patients susceptible to hypoperfusion if BP falls precipitously. The findings corroborate epidemiological data linking intravenous antihypertensive use in hospitalized noncardiac populations to increased risks of abrupt BP declines and poor outcomes, emphasizing caution.
While guidelines recommend BP control post-stroke, the optimal approach immediately post-EVT remains unclear. Variability in antihypertensive agents and dosing protocols further complicates management; hence, personalized BP targets considering cerebral hemodynamics may be warranted. Notably, BP remained dynamically similar between groups after the initial hours, suggesting early BP fluctuations rather than sustained hypotension may drive observed harm.
Limitations include the secondary, exploratory nature of the analysis, predominance of a single agent (nicardipine), and lack of data on adverse events like acute kidney injury. The study population was exclusively Korean, limiting broader generalizability. Nevertheless, these findings prompt critical reevaluation of routine intravenous antihypertensive use post-EVT.
Conclusion
Intravenous antihypertensive administration within 24 hours after successful EVT in acute ischemic stroke is associated with diminished functional independence and increased mortality at 3 months. These results highlight the need for individualized, cautious BP management post-recanalization to preserve cerebral perfusion and avoid hypoperfusion injury. Future prospective trials and pooled patient-level analyses are essential to refine antihypertensive strategies, identify optimal agents, and establish safe BP targets tailored to post-EVT pathophysiology.
References
Jung JW, Kim YD, Heo J, Lee H, Kim BM, Kim DJ, Shin NY, Joo H, Cho BH, Ahn SH, Park H, Sohn SI, Hong JH, Yun J, Song TJ, Chang Y, Kim GS, Seo KD, Lee K, Chang JY, Seo JH, Lee S, Baek JH, Cho HJ, Shin DH, Kim J, Yoo J, Baik M, Jung YH, Hwang YH, Kim CK, Kim JG, Lee IH, Choi JK, Lee CJ, Park S, Jeon S, Lee HS, Kim KH, Kwon SU, Bang OY, Heo JH, Nam HS; OPTIMAL-BP Trial Investigators. Association Between Intravenous Antihypertensives and Functional Outcome After Successful Endovascular Thrombectomy. Stroke. 2025 Sep;56(9):2503-2515. doi: 10.1161/STROKEAHA.125.051696IF: 8.9 Q1 B1.