Proton pump inhibitors (PPIs) are among the most commonly prescribed medications worldwide, with usage rising steadily. Approximately one in four adults use PPIs, often for extended durations exceeding one year. Despite their widespread acceptance as safe, concerns have emerged relating to serious adverse effects, notably intestinal dysbiosis and infections such as Clostridioides difficile infection (CDI). Originally, observational studies suggested that PPI use might double the risk of CDI by compromising gastric acid barriers and promoting colonization by pathogens. However, these studies suffered from significant heterogeneity and methodological limitations. This systematic review and meta-analysis aimed to rigorously examine whether PPI therapy is genuinely linked to an increased risk of CDI and other enteric infections, specifically focusing on evidence from randomized controlled trials (RCTs) to mitigate confounding biases inherent in observational research.
Study Design and Methods
The investigation adhered to PRISMA 2020 guidelines and the Cochrane Handbook recommendations. It was prospectively registered on PROSPERO (CRD42023403322). Eligible studies included adult patients receiving PPI therapy compared to placebo or other acid-suppressive agents, namely histamine-2 receptor antagonists (H2RAs) or potassium-competitive acid blockers, assessing outcomes including CDI, other enteric infections, and small intestinal bacterial overgrowth (SIBO).
A comprehensive search across MEDLINE, Embase, and CENTRAL until April 15, 2025, identified 19 RCTs suitable for inclusion. Data extraction and risk of bias assessment using RoB2 tools were conducted independently by reviewers. Risk ratios (RR) with 95% confidence intervals (CIs) were calculated using random effects meta-analyses to account for expected heterogeneity. The GRADE approach assessed overall evidence quality.
Key Findings
Clostridioides difficile Infection Risk
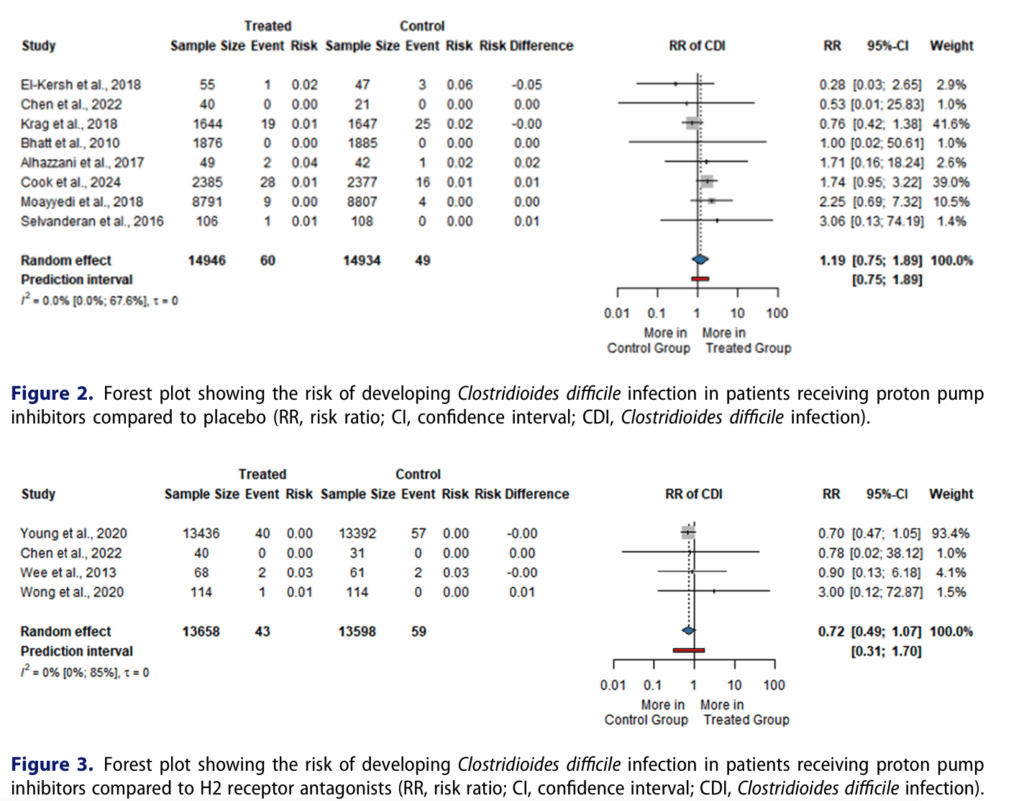
Eight RCTs (29,880 participants) comparing PPIs with placebo found no statistically significant increased risk of CDI (RR = 1.19; 95% CI: 0.75 to 1.89; I² = 0%). Similarly, four RCTs (27,254 participants) comparing PPIs with H2RAs revealed no difference (RR = 0.72; 95% CI: 0.49 to 1.07; I² = 0%). Additionally, three RCTs comparing PPIs with potassium-competitive acid blockers (1,645 participants) showed no significant difference (RR = 1.23; 95% CI: 0.43 to 3.55; I² = 0%). Overall, CDI incidence was low across groups, ranging between 0.3–0.4%.
Other Enteric Infections
Limited data from three RCTs suggested a modest but statistically significant increase in other enteric infections among PPI users compared to placebo (RR = 1.33; 95% CI: 1.01 to 1.75). However, comparisons with H2RAs and potassium-competitive acid blockers showed minimal or absent differences.
Small Intestinal Bacterial Overgrowth
Two RCTs examining SIBO rates reported higher prevalence among PPI-treated patients compared to non-users and H2RA recipients, with rates nearly doubling by various culture thresholds (RR ranges approximately 1.9 to 2.9). However, these studies had small sample sizes and variable diagnostic criteria, warranting cautious interpretation.
Expert Commentary
Previous observational data linking PPIs with increased CDI risk are likely confounded by indication bias, as patients prescribed PPIs tend to have comorbidities and risk factors for infection, including antibiotic use and hospitalization. RCTs, through randomization and controlled design, inherently minimize such biases, which could explain the discrepancy in estimates. Moreover, many RCTs involved short-term PPI use or prophylactic indications, whereas observational studies often assess chronic users, potentially contributing to differential findings.
While the meta-analysis underscores the general safety of PPIs with respect to CDI, it also highlights a possible increased risk for other enteric infections and SIBO, though data remain sparse and heterogeneous. Mechanistically, acid suppression diminishes gastric bactericidal activity, possibly facilitating overgrowth and colonization of gastrointestinal pathogens, but clinical impacts require further elucidation.
Limitations include the inability of included RCTs to primarily assess infection outcomes, varying diagnostic methods for CDI and SIBO, and heterogeneity in patient populations, dosing regimens, and treatment durations. The overall quality of evidence according to GRADE was very low due to indirectness and imprecision.
Conclusion
This systematic review and meta-analysis of randomized controlled trials demonstrates that proton pump inhibitor therapy does not significantly increase the risk of Clostridioides difficile infection compared to placebo or alternative acid-suppressive therapies. Although a modest increase in other enteric infections and small intestinal bacterial overgrowth was observed, the available data are limited and warrant cautious interpretation. Clinicians should continue to prescribe PPIs when clearly indicated, balancing the proven benefits against potential risks. Future large-scale, well-designed RCTs and rigorous observational studies are needed to further elucidate the gastrointestinal risks of long-term acid suppression, including geographic and strain-specific analyses of CDI.
References
Floria DE, Obeidat M, Váncsa S, Kávási SB, Földvári-Nagy L, Hegyi P, Veres DS, Drug VL, Erőss B. Proton pump inhibitors are not associated with an increased risk of Clostridioides difficile infection: a systematic review and meta-analysis of randomized controlled trials. Gut Microbes. 2025 Dec 31;17(1):2562341. doi: 10.1080/19490976.2025.2562341IF: 11.0 Q1 B1B1