Background
Stroke is a leading cause of long-term disability worldwide and substantially increases the risk of cognitive impairment and progression to dementia. Despite established cardiovascular rehabilitation protocols, there remains a crucial unmet need for effective prevention and treatment strategies targeting poststroke cognitive decline. Cardiorespiratory exercise (CRX) has been demonstrated to preserve brain health in general populations by increasing brain volumes and cognitive function, with prior evidence linking aerobic fitness to hippocampal volume (HV), a key region implicated in memory and cognition. However, direct evidence of CRX benefits on brain volume and cognition after ischemic stroke is limited, and safety concerns have constrained adoption in clinical practice.
Study Design
The Post-Ischemic Stroke Cardiovascular Exercise Study (PISCES) along with its adaptation, the Zoom Delivered Intervention Against Cognitive Decline (ZODIAC), conducted a phase 2b, assessor-blinded randomized clinical trial involving 107 adult ischemic stroke survivors recruited from four metropolitan health services in Melbourne, Australia. Participants were randomized 1:1 to receive either an 8-week CRX intervention consisting of prescribed intensity progressive aerobic and resistance training or an active control program highlighting balance and stretching exercises. The intervention commenced at approximately 2 months poststroke. Primary outcomes were assessed via longitudinal hippocampal MRI volumetry at baseline (2 months poststroke) and post-intervention (4 months poststroke). Secondary outcomes included executive function measured by the Trail Making Test Part B (TMT-B) at 12 months, adjusted for baseline performance and functional status. Safety parameters such as serious adverse events (SAEs) and recurrent vascular events were closely monitored.
Key Findings
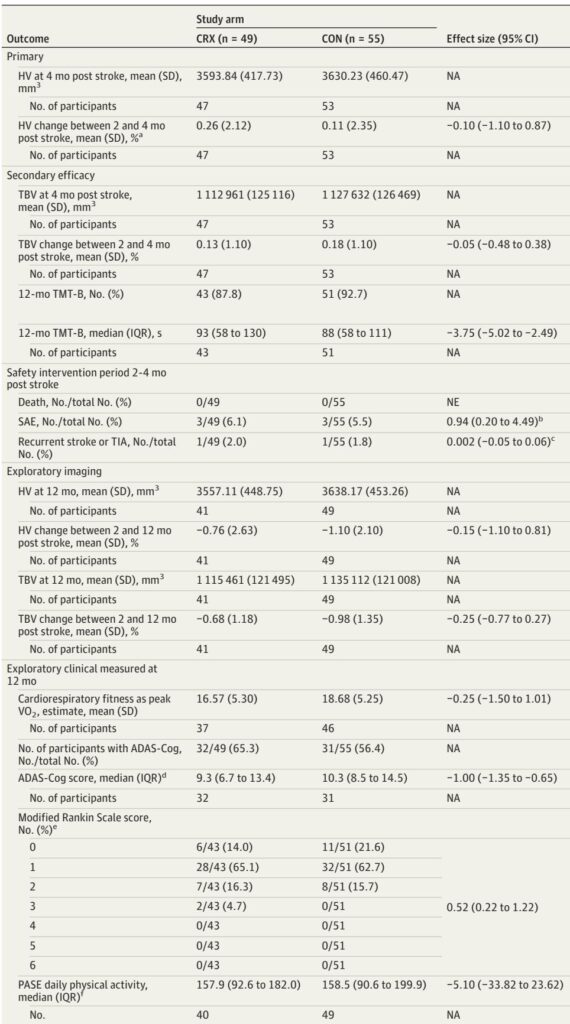
Out of 107 randomized participants, 104 initiated the intervention and were included in the modified intention-to-treat (mITT) analysis (49 CRX and 55 control). Baseline characteristics including age (mean 64 years), education level, and functional scores were balanced across groups, albeit with higher rates of atrial fibrillation in the control group and type 2 diabetes in the CRX group.
The primary outcome analysis revealed no statistically significant difference in relative HV change between the CRX and control groups over the 2-to-4 month poststroke interval (mean difference −0.10%; 95% CI, −1.10% to 0.87%; P = .83). Both groups exhibited less hippocampal atrophy than historical stroke cohorts, attributed in part to the active control design incorporating balance and stretching exercises that may also impact brain preservation.
Conversely, the CRX group demonstrated significantly better executive function at 12 months, with a median adjusted TMT-B completion time 3.75 seconds faster than controls (95% CI, −5.02 to −2.49 seconds), indicating preserved or enhanced processing speed and cognitive control. This was supported by exploratory improvements in global cognition assessed via the Alzheimer’s Disease Assessment Scale–Cognition subscale (ADAS-Cog).
Safety data confirmed the CRX intervention’s favorable profile, with no intervention-related deaths and comparable low rates of SAEs and recurrent strokes or transient ischemic attacks between groups.
Expert Commentary
This trial provides robust evidence that moderately intensive CRX initiated in the subacute phase after ischemic stroke is safe and may confer cognitive advantages at one year, despite the absence of measurable hippocampal volume preservation. The dissociation between volume and cognition may reflect that cognitive domains like executive function rely more on distributed neural networks, particularly frontoparietal white matter pathways, which are sensitive to aerobic training effects. Furthermore, the choice of an active control group may have attenuated observable differences in brain volume changes due to shared neuroplastic benefits from balance training and associated social factors.
While the study did not observe hippocampal volume benefits, it pioneers a scalable intervention framework that can be delivered both in-person and remotely, facilitating broader implementation. The inclusion of well-matched exercise professional contact time mitigates confounders linked to psychosocial engagement in rehabilitation.
Limitations include the small sample size, potential bias from baseline vascular risk imbalances, and underrepresentation of women limiting generalizability. Restrictions related to the COVID-19 pandemic impacted cognitive assessments and protocol consistency. Moreover, the clinical significance threshold for TMT-B improvements remains undefined.
Conclusions
CRX delivered two months post ischemic stroke is a safe and feasible intervention that may enhance cognitive outcomes at 12 months. Despite neutral effects on hippocampal volume, the cognitive benefits identified support incorporation of CRX into secondary stroke rehabilitation targeting cognitive preservation. Future phase 3 trials with larger, more diverse cohorts and longer follow-up are warranted to optimize exercise dosing, timing, and mechanistic understanding. Given the increasing global dementia burden and modifiable risk factors, CRX offers a promising, low-risk strategy for neurorehabilitation poststroke with potential population health impact.
References
Brodtmann A, Churilov L, Adkins K, et al; PISCES-ZODIAC Investigators. Poststroke Cardiorespiratory Exercise for Brain Volume and Cognition: A Randomized Clinical Trial. JAMA Netw Open. 2025 Aug 1;8(8):e2528907. doi:10.1001/jamanetworkopen.2025.28907. PMID: 40856999; PMCID: PMC12381666.